World Health Organization

WORLD HEALTH ORGANIZATIION – This report provides a global overview of the monkeypox epidemiological situation as reported to WHO as of August 18 2022. The report focuses on laboratory confirmed cases1 as defined by the WHO’s working case definition published in the Surveillance, case investigation and contact tracing for monkeypox interim guidance. Note that countries may use their own case definitions separate from those outlined in the above document. This report should be considered in the context of other WHO information products associated with the 2022 monkeypox outbreak, and monkeypox in general:
- The biweekly Situation Report provides a comprehensive update of the monkeypox situation and response activities across a variety of domains such as epidemiology, clinical management and communications, replacing the previous Disease Outbreak News format;
- The Emergency Dashboard provides the latest daily data on total cases and deaths of monkeypox, as well as other events and emergencies to which WHO is responding;
- This global epidemiological report provides in-depth epidemiological information about the monkeypox situation, based primarily on case report forms provided by Member States to WHO under Article 6 of the International Health Regulations (IHR 2005).
Links to these products can be see in more detail HERE.
Since 1 January 2022, cases of monkeypox have been reported to WHO from 94 Member States across all 6 WHO regions. As of August 18, 2022 at 17h CEST, a total of 39,110 laboratory confirmed cases and 191 probable cases, including 12 deaths, have been reported to WHO. Since 13 May 2022, a high proportion of these cases have been reported from countries without previously documented monkeypox transmission. This is the first time that cases and sustained chains of transmission have been reported in countries without direct or immediate epidemiological links to areas of West or Central Africa.

With the exception of countries2 areas of West and Central Africa, the ongoing outbreak of monkeypox continues to primarily affect men who have sex with men who have reported recent sex with one or multiple partners. At present there is no signal suggesting sustained transmission beyond these networks.
Confirmation of one case of monkeypox, in a country, is considered an outbreak. The unexpected appearance of monkeypox in several regions in the initial absence of epidemiological links to areas in West and Central Africa, suggests that there may have been undetected transmission for some time.
WHO assesses the global risk as Moderate. Regionally, WHO assesses the risk in the European Region as High and as Moderate in the African Region, Region of the Americas, Eastern Mediterranean Region and the South-East Asia Region. The risk in the Western Pacific Region is assessed as Low-Moderate. The IHR Emergency Committee on the multi-country outbreak of monkeypox held its second meeting on 21 July 2022. Having considered the views of committee members and advisors as well as other factors in line with the International Health Regulations (2005), the WHO Director-General declared this outbreak a public health emergency of international concern and issued temporary recommendations in relation to the outbreak.
Global situation update
The number of weekly1 reported new cases globally has increased by 20.3% in week 32 (08 Aug – 14 Aug) (n = 7,477 cases)compared to week 31 (01 Aug – 07 Aug) (n = 6,217 cases). The majority of cases reported in the past 4 weeks were notified from the Region of the Americas (57.9%) and the European Region (41%).
The 10 most affected countries globally are: United States of America (n = 12,743), Spain (n = 5,792), Germany (n = 3,242), The United Kingdom (n = 3,195), Brazil (n = 3,184), France (n = 2,749), Canada (n = 1,091), Netherlands (n = 1,029), Peru (n = 867), and Portugal (n = 770). Together, these countries account for 88.6% of the cases reported globally.
In the past 7 days, 36 countries reported an increase in the weekly number of cases, with the highest increase reported in United States of America. 17 countries have reported no new cases in the past 21 days.
In the past 7 days, 2 countries reported their first case. countries which reported their first case in the past 7 days are: Monaco (12 August), Iran (Islamic Republic of) (18 August).
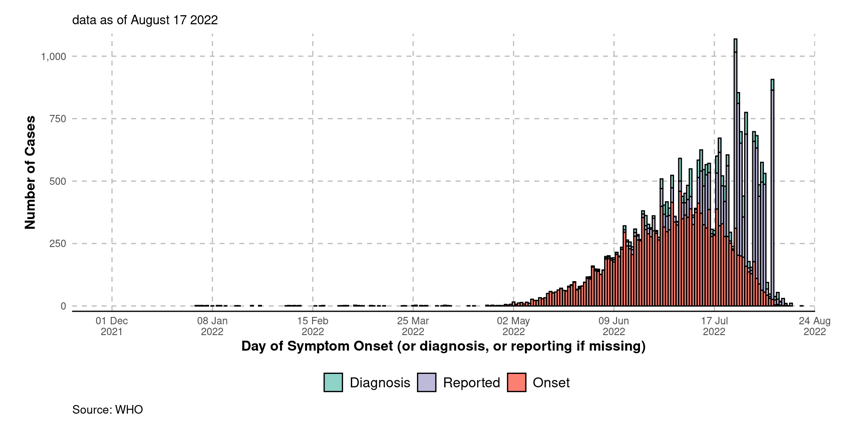
Global data are data collected by public sources. These data are largely aggregated cases that have been reported from open and official country sources. The below epidemic curve shows the aggregated number of cases by week according to the date of case reporting.
Detailed case data
Detailed case data are acquired via direct reporting of case based data via WHO Member States. Data from cases are reported1 according to the WHO minimum dataset under the International Health Regulations (IHR 2005) Article 6, and subsequently aggreagated and presented below. Note that completeness of records is variable, meaning denominators for each output may be different from one another. All of the following is derived from the detailed case data, and as a result, overall numbers may not be reflective of figures shown with aggregate case numbers. All detailed cases shown are confirmed cases, where the reporting date occured after 01 January 2022.
- Note that a small number of detailed case reports are constructed from official public reports about individual cases.
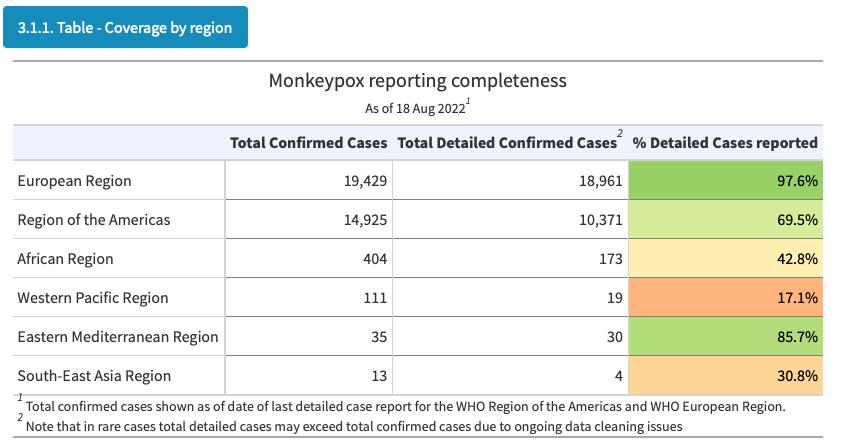
Reporting coverage
The detailed case dataset was last updated on August 17 2022. As of this date, the total number of detailed confirmed cases reported is 29,558, representing 84.7% of all aggregated cases reported.
The table below indicate the reporting coverage between reported aggregated confirmed cases and detailed confirmed cases by countries and per region.
Note that for all tables below, in order to best align modes of reporting, total confirmed cases are shown as of:
- The most recent Friday (12 August) for data in the Region of the Americas.
- The most recent Tuesday (16 August) for data in the European Region.
Total cases shown fully as of 18 August are shown in the global trends section.
Trends in cases
Trends in cases are shown for all submitted detailed cases. These are shown by:
- Date of symptom onset
- Date of lab or clinical diagnosis (if date of symptom onset is not available)
- Date of reporting (if date of symptom onset and date of diagnosis are not available)
Note that reporting of detailed cases is subject to some delay. The epidemic curves shown are not right censored, and therefore trends in the most recent 1-3 weeks should be interpreted with caution. It should be additionally noted that date of report does not reflect the date of reporting to WHO, but rather reporting to national or regional authorities.
Delay between date of onset and date of report were calculated for all countries where reporting quality passed minimum quality checks. Delays were only shown when the time between onset and reporting was between -5 and 40 days.
- Median delay between onset and reporting was 7 days
- The interquartile range between onset and reporting was 4-10 days.
Case profile (overall)
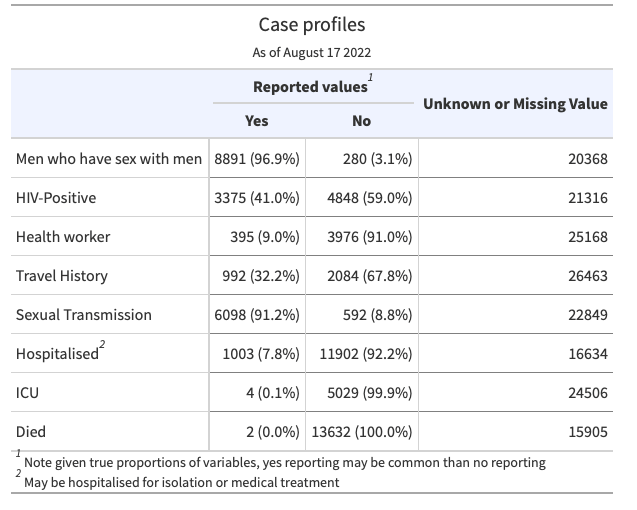
As shown below, and stated previously, the ongoing outbreak is largely developing in men who have sex with men (defined as homosexual or bisexual males in detailed case forms) networks. In the following analyses, we have re-coded men reported as bisexual as men who have sex with men. Note that reported sexual orientation does not necessarily reflect who the case has had recent sexual history with nor does it imply sexual activity. Generally, severity has been low, with few reported hospitalisations and deaths:
Key features of these cases are as follows:
- 98.5% (17681/17943) of cases with available data are male, the median age is 36 years (IQR: 30 – 43).
- Males between 18-44 years old continue to be disproportionately affected by this outbreak as they account for 76.5%of cases.
- Of all cases with available data, 1.5% (262/17943) are female:
- The majority of of these cases are reported from the European Region (177/262; 68%) and the African Region (61/262; 23%)
- Of the cases where sexual orientation is reported, the majority are Heterosexual (76/82; 93%).
- The most commonly reported exposure setting is in a household (20/56; 36%), and the most common form of transmission is via sexual encounters (49/85; 58%)
- Of the 21,042 cases where age was available, there were 107 (0.5%) cases reported aged 0-17, out of which 26 (0.1%)were aged 0-4:
- The majority of these cases are reported from the African Region (65 /262; 61%).
- Of the children reported, 0 have reported exposure in a school setting.
- Among cases with known data on sexual orientation, 96.9% (8891/9171) identified as men who have sex with men. Of those identified as men who have sex with men, 82 / 8891 (0.9%) were identified as bisexual men.
- Among those with known HIV status 41.0% (3,375/8,226) were HIV-positive. Note that information on HIV status is not available for the majority of cases, and for those for which it is available, it is likely to be skewed towards those reporting positive HIV results.
- 395 cases were reported to be health workers. However, most were infected in the community and further investigation is ongoing to determine whether the remaining infection was due to occupational exposure.
- Of all reported types of transmission, a sexual encounter was reported most commonly, with 6,101 of 6,693 (91.2%)of all reported transmission events.
- Of all settings in which cases were likely exposed, the most common was in party setting with sexual contacts, with 2,221 of 3,652 (60.8%) of all likely exposure categories.
Note that the proportions shown below should be interpreted with caution. When considering some variables, it is more likely that a yes response will be obtained when compared to a no response after consideration of true proportions of these factors. This is most likely to be true for variables where reported answers can only be yes or no, such as HIV status, health worker status, travel history, hospitalisation, ICU, and death.
Case profile (excluding men who have sex with men)
The following outputs apply to cases that are not men who have sex with men, and sexual orientation is known. Other categories of sexual orientation that are reportable are:
- Heterosexual
- Lesbian (women who have sex with women)
- Other
As stated above, men who have sex with men in this case refers to those who have a reported sexual orientation of men whi have sex with men, and men reported as bisexual. As above, note that reported sexual orientation does not necessarily reflect persons who the case has had recent sexual history with nor does it imply sexual activity. Up until this point in time, the 2022 multi-country Monkeypox outbreak has been overwhelmingly concentrated in networks of men who have sex with men For this reason, understanding events in which individuals of other sexual orientation have acquired monkeypox is important to monitor potential of sustained spillover into the general population.
- 70.1% (192/274) of cases with available data are male; the median age is 34 years (IQR: 28-43).
- Males between 18-44 years old account for 53.6% of cases.
- Among those with known HIV status 9.1% (21/230) were HIV-positive. Note that information on HIV status is not available for the majority of cases, and for those for which it is available, it is likely to be skewed towards those reporting positive HIV results.
- 3 cases were reported to be health workers. However, most were infected in the community and further investigation is ongoing to determine whether the remaining infection was due to occupational exposure.
- Of all reported types of transmission, sexual encounter was reported most commonly, with 102 of 130 (78.5%) of all reported transmission events.
- Of all settings in which cases were likely exposed, the most common was in party setting with sexual contacts, with 28 of 88 (31.8%) of all likely exposure categories.

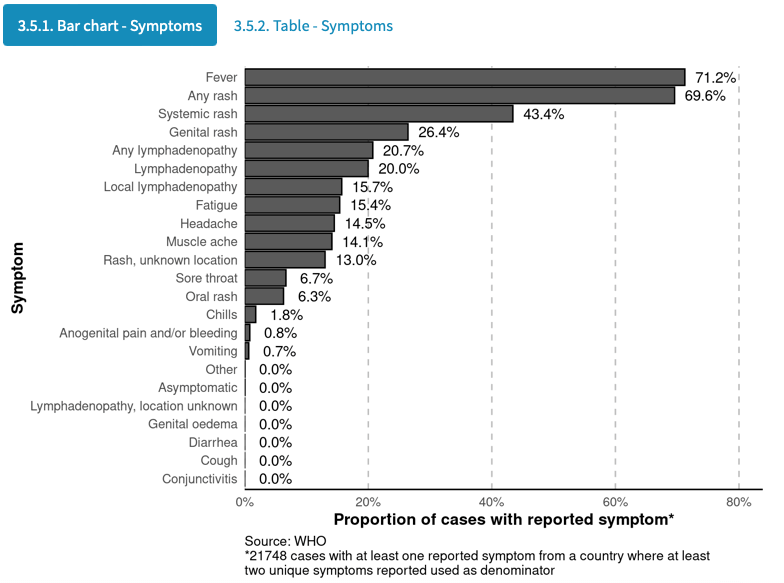
Symptomatology
Although most cases in current outbreaks have presented with mild disease symptoms, monkeypox virus (MPXV) may cause severe disease in certain population groups (young children, pregnant women, immunosuppressed persons)
Among the cases who reported at least one symptom, the most common symptom is fever and is reported in 71% of cases with at least one reported symptom. Note that identifying true denominators for symptomatology is difficult due to a general lack of negative reporting and symptom definitions that may vary between countries’ reporting systems.
A bar chart and table showing symptoms is shown below. Here any rash refers to one or more rash symptoms (systemic, oral, genital, or unknown location), and any lymphadenopathy refers to either general or local lymphadenopathy.